Celebrating My Two-Year Stoma-Versary
I used to feel like I couldn’t say, “my ostomy bag saved my life,” because I didn’t get my ostomy bag for the same reasons a lot of people do. Some of the most common reasons people need ostomies are for inflammatory bowel disease (IBD), acute infections like diverticulitis, or colon cancer – conditions with obvious pathology that can be seen and measured in ways to assess the risk of “to bag or not to bag.” My conditions, though, are much less obvious or measurable, let alone well-known in the medical field.
If you’re here because you have Ehlers-Danlos syndrome (EDS) and something about my experience sounds familiar, I’m glad you’re here. If you’re a medical provider who has encountered a patient like me but was stumped, keep reading.
What Is an Ostomy
Before we get into it: an ostomy is a surgical procedure that creates an opening (called a stoma) in the abdominal wall, allowing waste to exit the body into an external pouch rather than through the traditional route (your rear-end).
There are different types of ostomies:
-
Colostomy diverts the large intestine
-
Ileostomy diverts the small intestine
-
Urostomy diverts urine
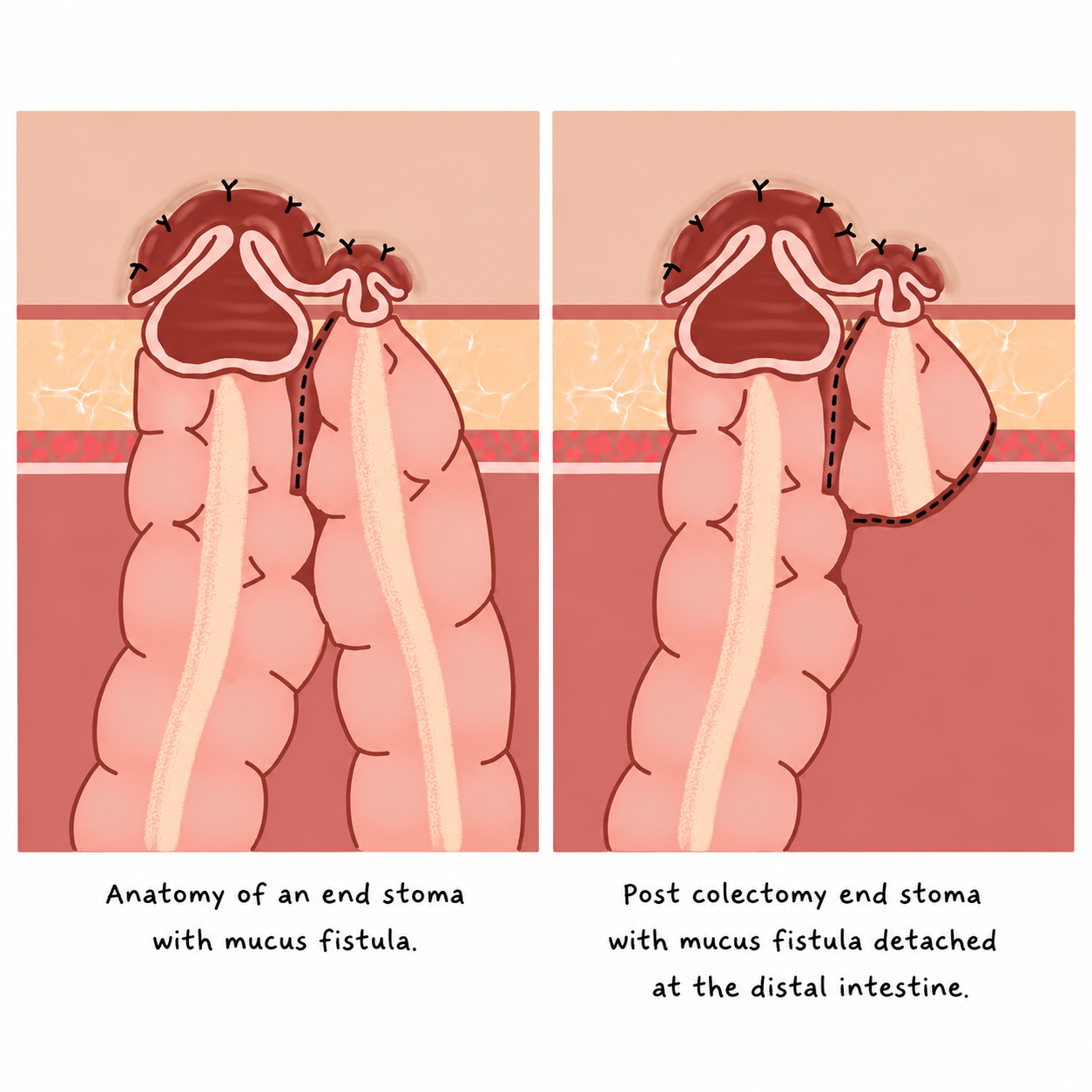
As I have a permanent end ileostomy, my small intestine was brought to the surface of my abdomen, and my colon has since been removed. This is opposed to a loop ostomy, where, quite literally, a loop of bowel is brought to the surface and often used in cases where the ostomy is intended to be temporary. There is also an end stoma with mucus fistula, also sometimes called an end-loop stoma, which is used in cases like mine, where the large intestine remains in the body at the same time that an end stoma was created.
Why Does This Matter For EDS?
For people unfamiliar with EDS: Ehlers-Danlos syndrome is a group of connective tissue disorders. Connective tissue is essentially the scaffolding of your body. It holds your organs, joints, skin, and blood vessels, giving them structure. EDS is multisystemic, meaning it affects multiple areas of the body and extends far beyond what many people assume is “just” a bendy joint disorder. For me, one way my EDS manifested was in my gastrointestinal tract.
A Lifetime of “Just Constipation”
I don’t remember a time before the stomach pain. From elementary school hallways, doubled over waiting for a wave to pass, to middle school bathrooms, sitting too long on a toilet that never produced anything, to high school, learning to turn my poop issues into a joke to avoid the inevitable awkwardness.
By college, it had escalated from embarrassing to severely debilitating, like afraid to leave my house kind of debilitating. I tried everything that was recommended by my doctors over the years:
-
Prescription laxatives and motility medications
-
Dietary changes: more fiber, elimination diets
-
Increased hydration
-
Pelvic floor physical therapy
-
Abdominal massage to manually stimulate movement
-
Enemas and suppositories
-
Manual digital evacuation (called splinting – inserting a finger vaginally to press against the rectal wall to help stool pass)
My symptoms, at their worst, looked like:
-
Going 57 days without a bowel movement
-
Recurrent bowel obstructions
-
Attacks of pain so severe I was rocking back and forth, digging my nails into my skin, barely able to breathe
-
Pain hitting without warning, in class, at work, in public, and with no way to explain it to the people around me
-
Severe bloating and lower abdominal distention that worsened when upright
-
Chronic nausea, inability to eat, malnutrition
-
Ability to see physical lumps of stool in my lower abdomen
-
Sitting on the toilet for hours with no productivity
-
Lack of regular stool sensations mixed with urgency
-
Inability to evacuate stool even if it was ready
The Road to a Diagnosis (And Why It Took So Long)
When a gastrointestinal (GI) specialist finally took me seriously, the testing revealed another diagnosis or layer of what was happening and we were able to connect the issues that everyone before then had overlooked (whether intentionally or not).
The Cascade of Testing
-
Sitz marker study: swallowing small markers and tracking how they moved (or didn’t) through my colon via X-ray
-
Anorectal manometry: measuring the pressures and muscle coordination in my rectum and anal sphincters via a probe inserted into my back end
-
MR defecography: imaging of how my pelvic floor and rectum functioned during defecation via MRI
-
Gastric emptying study: tracking how quickly my stomach emptied
-
Barium enema: filling my colon with barium through an enema and taking upright images to show structure and positioning
-
Upper GI with small bowel follow-through: during this study, gastroptosis (stomach prolapsing) was also evident on my imaging. I had to provide the radiologist with research guidance to correctly report the finding.
Throughout all of these discoveries, I had to guide the radiologist and surgeons, more than once, to get the answers I needed and deserved.
What the Testing Revealed
-
Visceroptosis: Visceroptosis is an umbrella term to describe when one or more abdominal organs prolapse when the body is upright. A few small-scale studies show an association between visceroptosis and connective tissue disorders, however, the condition remains underresearched and underdiagnosed. The subtypes of visceroptosis include:
-
Gastroptosis: displacement of the stomach into the pelvis beyond the top of the pelvic bones
-
Enteroptosis: displacement of the small intestines into the pelvis
-
Colptosis: abnormal displacement of the colon
-
Hepatoptosis: the liver is displaced downward from its normal position in the upper right abdomen
-
Nephroptosis: kidney drops more than 5 cm (or two vertebral bodies)
-
-
Paralyzed and Redundant Colon / Colonic Dysmotility: My colon was too long and twisted and no longer had sufficient peristalsis to move stool on its own. When my colon was removed, it had zero muscular structure.
-
In people with EDS, disrupted neuromuscular signaling and structural laxity can impair gut motility over time. Severity and disruption of daily functioning varies widely. A recent study reported that 43% of hEDS participants were diagnosed with constipation, and 6.8% had specified colon dysmotility. Less than 1% reported visceroptosis, however it is likely underdiagnosed due to lack of knowledge in the medical field and the need for upright imaging.
-
-
Pelvic Floor Dysfunction: I have pelvic organ prolapse and dyssynergia, which causes issues with stool evacuation. Basically, the muscles that are supposed to coordinate to let you go were working against each other instead.
The Decision
My colorectal surgeon told me in our first virtual appointment that I would likely need a permanent ostomy bag. I had already done enough research to not be entirely shocked but the word “permanent” still gave me a little bit of whiplash.
The anxieties I had were real:
What does life actually look like with a bag?
Will it leak? Will I smell? Will people notice?
What about clothes, swimming, intimacy, attraction?
Will my contamination OCD spiral?
How will the transition be from never having poop to always having poop?
What if it doesn’t even help?
What I kept coming back to, though, was the reality of my current existence. The idea of a bag wasn’t more frightening than what I was already living, but I would have moments of self-doubt, and if I’m naming it for what it truly was: self-gaslighting.
Surgery, Recovery, and the Honest Version
I first had surgery to create my stoma and I felt immediate relief. I felt so much better and started to thrive for the next year. However, I still had my colon which at this point was just dead weight. One year after my stoma creation, I had my colon removed. That one year was even further reassurance that I had made the right choice. The leftover stool in my colon continued to very slowly make its way out of my body up until the week before my total colectomy.
My colectomy was over ten hours, and my colon (all seven-plus feet of it) was removed. The recovery was not clean or linear. I’ll spare you the details as anyone with EDS knows healing can never go as planned, and I had to advocate through all of it, from a hospital bed.
But here is what I also know: the moment my ostomy was functional, my body felt different. The bloating and heaviness that had been a constant companion for decades resolved.
Life on the Other Side
Not long after surgery, I started sewing ostomy bag covers. Each cover is hand-cut and sewn, completely unique. What started as a personal creative outlet became a small business to give others the chance for confidence that I found, and it has led me to amazing places.
I do want to be honest with you: living with an ostomy is hard sometimes. Leaks happen. Skin gets irritated. There are moments of grief, especially early on. It is okay to feel everything you are trying to process through your journey, and is actually part of the healing process. There is always a community you can turn to when you need support.
When I was first researching visceroptosis, the Facebook support group had fewer than 100 members. The isolation of having a condition almost no one has heard of, where you have to hand your radiologist research papers just to get the imaging reported correctly, is its own kind of exhausting.
My Instagram platform became a place where I could document what actually living with an ostomy looks like. I’ve talked about it on podcasts. I’ve written for medical advocacy publications. And this year, I traveled to Kenya with Campaign 52 to provide ostomy education, supplies, and resources at a women’s hospital specializing in pelvic and colorectal disorders. I never would’ve thought going through something that was so scary and intimidating could’ve brought me where I am now, and I can confidently say that my ostomy bag saved my life.
Key Takeaways
-
EDS is a multisystemic condition that can affect gastrointestinal function in multiple, overlapping ways.
-
Visceroptosis is underdiagnosed and may require upright imaging to visualize: a protocol that is not standard and often requires patient self-advocacy to obtain.
-
Ostomy bags do not mean the end of a full life. Travel, exercise, intimacy, creativity, community, and professional work all remain possible, and ostomies can give that back to you.
-
Treatment efficacy varies from person to person. While this intervention worked for me, everyone with EDS is very different. Some cases are well managed with very conservative treatments, others require other interventions.
-
Community matters. Finding people who share your experience is irreplaceable.
What This Means for You
If you are an EDS patient with unexplained and treatment-resistant GI symptoms, please know you are not imagining it, and “just constipation” is not less excruciating or serious just because it isn’t as visible and measurable.
If you are a medical provider: when your EDS patient describes a lifetime of GI dysfunction that hasn’t responded to standard interventions, please investigate the structural or “rare” possibilities. These are not exaggerated symptoms.
And if you are someone newly facing the possibility of a bag, or freshly post-op and grieving or scared or both: I see you. On the other side of it, there is a version of your life that is actually livable.

Tayler Goectau, Author,
Clinical Research Coordinator,
Disability Advocate
@distaaybled
May 28, 2026
Disclaimer: The experiences described in this article are those of the author and may not reflect the experiences of all people with EDS, gastrointestinal dysmotility, visceroptosis, or ostomies. Discussion of diagnostic testing, surgical interventions, and treatment outcomes is provided for educational purposes only and should not be interpreted as medical advice. Readers should consult their healthcare team regarding their individual circumstances.